⚀ 1. Webpage plan.
≻ This webpage begins with a broad overview of IBM presented in Section 2.
≻ Section 3 presents the common complications seen as IBM progresses and some other diseases that commonly occur along with IBM.
≻ Section 4 briefly mentions diagnosis.
Note: this is not a disease that you can diagnose from the Internet!
≻ Section 4 concludes with a discussion of treatment. Videos from Johns Hopkins provide excellent descriptions (linked).
≻ Section 5 discusses the causes of IBM and highlights the latest scientific research on IBM that is intended more for doctors.
≻ Section 6 includes an overview of the physical accommodations and adaptations usually required as IBM progresses.
≻ Section 7 looks at the psychological aspects of dealing with a chronic, progressive, and debilitating illness like IBM.
≻ Finally, section 8 presents links that will take you to further explanations, discussions, and resources.
≻ There is a tremendous amount of information on this webpage and my suggestion is that you slowly work your way through it.
⚀ 2. Overview.
⚂ If you have been diagnosed with inclusion body myositis here is what you need to know to begin with.
⚂ Brochure: Myositis Support and Understanding (MSU)
⚁ 2.1 Key information for new patients.
⚂ 2.1.1 General Aspects.
⚃ Inclusion body myositis (IBM) is a rare, debilitating, chronic, and progressive muscle disease.
⚃ The disease strikes people later in life, usually developing after age 40. Most people develop IBM between the ages of roughly 50 and 70.
⚃ Of every hundred patients, roughly 67 will be men, and 33 will be females.
⚃ Although people may feel the disease “goes up and down,” research has shown that it does not; it is not known to go into remission.
⚃ Over time, the disease will advance and weakness will get progressively worse.
⚃ IBM likely has genetic predispositions, but it is not an inherited disease; the disease occurs randomly.
⚃ In the past it was often referred to as sporadic inclusion body myositis (sIBM) – this term is still used sometimes but is no longer recommended.
⚃ The disease affects people in different ways, and at different
rates, so you cannot compare yourself with others.
≻ The disease starts in different people at different ages.
≻ The rate at which the disease progresses varies widely in
patients.
≻ The disease may impact men and women differently.
≻ The disease may impact black patients differently.
≻ It is clear that severity varies widely – there
are very mild cases and, as well, there are severe cases.
≻ For some reason, the impact of IBM may differ based on the age
when you developed symptoms.
⚃ IBM is considered one of the most challenging muscle diseases to
diagnose.
≻ On average it takes 5 years to get a diagnosis.
⚃ IBM is not responsive to treatment.
⚂ 2.1.2 Impact on muscles.
⚃ IBM is a disease that primarily impacts and kills skeletal
muscle cells, eventually weakening the muscles involved.
≻ As more muscle cells are killed, the muscle becomes weaker, and
more and more function is lost.
≻ It does not affect the nerves.
≻ It has been conventionally said that the heart is not affected
by IBM. Research now shows that the risk of a heart attack (myocardial infarction) is some 4 to 6 times
higher in patients who have IBM (Beecher et al., 2025).
⚃ As IBM advances and patients get older, they may need more help to accomplish the day-to-day functions of life like getting up in the morning, showering, going to the bathroom, eating, etc.
⚃ The disease usually leads to severe disability of mobility and often necessitates using assistive mobility devices, for example, a wheelchair and a lift to transfer you in and out of bed.
⚃ Muscles tend to be impacted in a fairly characteristic
pattern.
≻ Different muscle groups are affected at different rates and
times.
≻ ≻ Some people first show weakness in the muscles that control the hands
and arms. As a result, gripping objects becomes difficult as finger strength diminishes. Using keys,
opening doors, and other tasks requiring dexterity become challenging. Lifting things and raising your
arms over your head may become a challenge (e.g., putting an item on a high shelf.)
≻ ≻ Some people first develop weakness in the leg muscles. Climbing
stairs, rising from chairs and walking are impacted. Falls become frequent.
≻ ≻ Others may show weakness in swallowing as a first symptom. This
serious symptom may lead to choking.
⚃ In the past, doctors advised against exercise. Today, in the early stages after diagnosis, a supervised and individualized exercise program is recommended, focussing on unaffected muscles.

⚂ 2.1.3 Common complications.
⚃ A common serious complication is weakness in swallowing
(dysphagia) that can cause choking or aspiration (taking food into the lungs), causing pneumonia
(sometimes a cause of death).
≻ Swallowing involvement is a critical factor that should be
investigated after an IBM diagnosis.
≻ Swallowing involvement can be identified, monitored, and
treated.
⚃ Another serious possible complication is respiratory impairment
caused by weakness of the diaphragm.
≻ Respiratory involvement is a critical factor that should be
investigated after an IBM diagnosis.
≻ Respiratory dysfunction can be identified, monitored, and
treated.
⚃ Many IBM patients report having pain, often severe
pain.
≻ Research has generally either said that IBM is pain-free or has
not addressed the issue of pain at all.
≻ In a 2022 study done by Bhashyam (and others), they looked at
pain in IBM and found that of “113 IBM patients, some 106 (81%) reported pain, and of this group,
88 took pain medication (83%).
≻≻ Of the 88, 45 (62.5%) took opioids, and 82 (93.2%) took
non-opioid pain medication.”
⚂ 2.1.4 Research into the causes of IBM.
⚃ Despite extensive research efforts, the underlying cause of IBM remains unknown.
⚃ Research is gradually increasing our understanding of the factors involved in IBM but today there is no consensus about a cause.
⚃ The current consensus is that multiple factors likely contribute to the cause, including genetic predispositions and factors linked to aging.
⚃ Not knowing the cause makes developing a treatment very challenging.
⚃ The major abnormalities seen in the muscle fall into three categories: immune system attacks on muscle cells, degenerative aspects involving proteins in the muscle cells, and defects in the Mitochondria of these cells.
⚃ Researchers have looked at autoimmune factors and protein degeneration as possible causes, however today, the role of mitochondria are increasingly implicated.
⚃ An antibody – Anti-cN1A – directed against cytosolic
5'-nucleotidase 1A (cN1A) is found in the blood of about 50% of IBM patients.
≻ Because not all IBM patients show this antibody and because
other diseases may produce it, it should not be used as a standalone test.
≻ If you have the antibody, it is suggestive of having IBM; if you do not have the antibody, you could still
have IBM.
≻ Also, researchers have not been able to consistently show any
significant differences between people who have these antibodies compared to people who do not.
⚂ 2.1.5 Review Articles.
⚂ Naddaf, E. (2025). Inclusion Body Myositis. Continuum, 31(5), 1372-1384. Click for detailed information on this article.
⚂ Krause, K., Ruck, T., & Kleefeld, F. (2025). Inclusion body myositis – what are new lines of pathogenesis and therapy? Current Opinion in Neurology. Available Here.
⚂ Anderson and Lloyd (2024).
≻ IBM presents itself in various ways in different
patients.
≻≻ Studies of IBM patients appear to show differences based on age of
onset, between males and females, and between Black and White patients.
≻≻ A group of early-onset patients has been identified – the
age of symptom onset is about 36 years.
≻ IBM occurs in about 182 per million people over the age of
50.
≻ Swallowing and breathing difficulties can arise
independently of the degree of limb weakness.
≻≻ Swallowing problems may eventually impact two-thirds of patients
and are often the initial symptom; the first symptom seen in 23% of women and 10% of men.
≻ 50% of IBM patients have another autoimmune disease, often
rheumatoid arthritis or Sjögren’s syndrome.
≻ A study of IBM patients showed that 60% had a reduced lung
volume (when the lungs cannot reach their normal capacity) when first seen.
≻≻ Patients with respiratory involvement (ventilatory pump
impairment) were more likely to be unable to walk. (This first shows itself as not being able to breathe
enough at night, often with shortness of breath caused by diaphragm weakness. Eventually, high carbon
dioxide levels appear in the blood during daytime hours.)
≻ More than 35% of IBM patients report depression and
anxiety.
≻ The anti-cN-1A antibody cannot be used in diagnosis –
better and more standardized antibody testing must be developed.
≻ Facial weakness may be present and may be associated with
problems swallowing.
≻ Outcome measures are essential, especially when conducting
studies.
≻≻ The IBMFRS is a common measure but requires more research.
≻≻ MRI and ultrasound are being researched as ways to measure
IBM.
≻ Exercise can improve muscle strength and aerobic
activity.
≻ Palliative care is under-utilized in IBM cases.
⚁ 2.2 Impacts and more.
⚂ 2.2.1 Impact on muscles.
⚃ Depending on how you are affected, you will face various physical challenges:
⚄ If the disease affects your arms, you may have problems picking
up objects and using your fingers.
≻ Eventually it may become difficult to raise your arms.
⚄ If the disease affects your legs, you may fall frequently, have
problems climbing stairs, etc.
≻ Eventually you may not be able to walk and may require the use
of a wheelchair.
⚄ If the disease affects your throat, you may have trouble swallowing.
⚄ If the disease affects the breathing muscles, you may have problems getting enough air, especially at night.
⚃ Before we go any further, it is very helpful to know these very basic terms that are used in describing the movements of the body.
⚄ Two very common terms describing the action of muscles in moving the body are extension and flexion (From).

⚄ Finger flexion describes the movement of the fingers, driven by
the flexor muscles located in the forearm and connected by tendons, to bend the fingers inward toward
the palm, as in closing the hand and making a fist.
≻ This movement is often severely compromised by IBM.

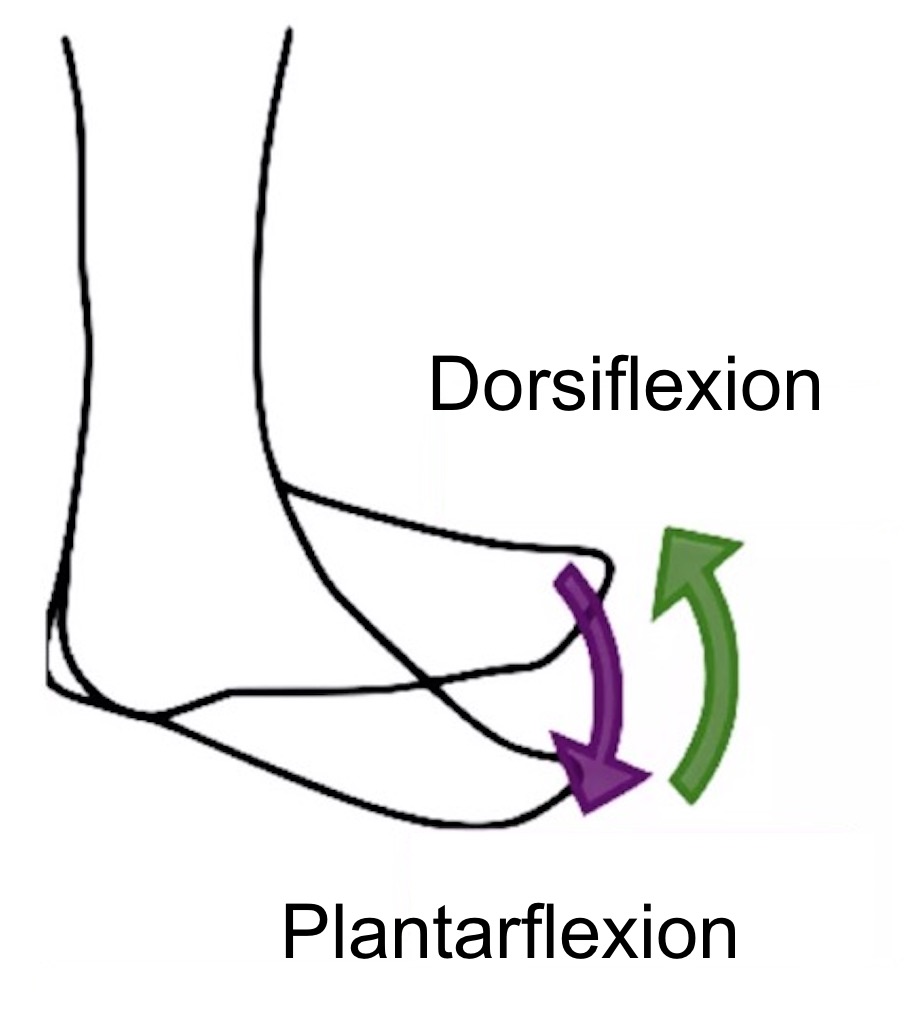
⚄ A very common problem in IBM is difficulty lifting the toe when
walking or stepping up.
≻ This is called dorsiflexion (from
https://biologydictionary.net/plantar-flexion/)
≻ This is also called “foot drop.”
⚃ This illustration shows the common muscle groups impacted (blue) and the most common and serious potential complications (orange) (after Greenberg, 2019).
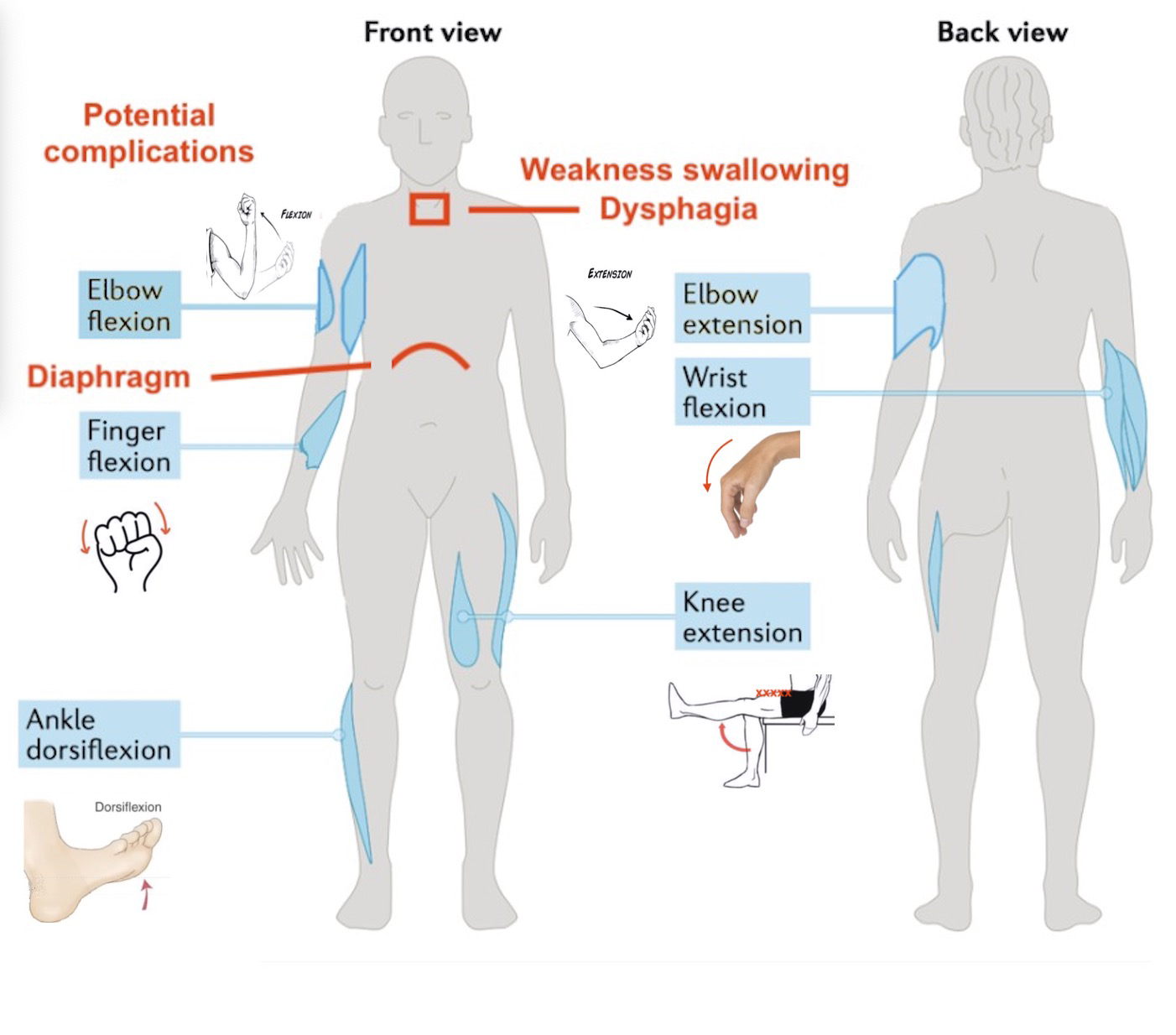
⚃ It is common to see asymmetry where one side of the body is impacted more than the other.

⚂ 2.2.2 Tendon transfer.
⚃ There are no muscles in the fingers. The muscles that control the fingers are in the forearm between the elbow and the wrist. They are connected to the fingers through tendons that pass through the carpal tunnel on the palm side of the wrist. The idea behind tendon transfer is to move tendons from weak muscles in the arm and attach them to stronger arm muscles to improve hand function.

⚂ 2.2.3 Common questions IBM patients ask.
⚂ 2.2.4 Classification of IBM.
⚂ 2.2.5 Blood tests in IBM.
⚂ 2.2.6 Impact on lifespan.
⚃ IBM does not directly lead to death and is not classified as a life-threatening disease.
⚃ If you have IBM, it tends to shorten your life by an average
of three years compared to the population.
≻ Statistically, the median age of death is 84 compared to 87.5 in
the population (Naddaf et al., 2021; Shelley et al., 2021).
≻ The cause of this appears to be related to the complications of
IBM, primarily, respiratory issues – aspiration.
≻ Also, falls are a risk factor.
⚃ The most common causes of death in IBM patients are complications due to respiratory failure and aspiration pneumonia.
⚃ Ongoing monitoring and awareness of dysphagia and respiratory involvement are highly recommended.
⚂ 2.2.7 Brief History of IBM: A few highlights.
⚂ 2.2.8 How common is IBM? / IBM and aging.
⚂ 2.2.9 Genetic predisposition of IBM.
⚂ 2.2.10 IBM and just getting old.
⚃ As people get older they often encounter various health
issues.
≻ For example, problems with vision and hearing increase with
age.
≻ Body pain in the back and neck become more common.
≻ As well, with age, depression is more common.
≻ Problems concentrating and forgetfulness may increase.
≻ Patients often ask if these types of issues are caused by their
IBM.
≻ The short answer is usually no, most often they are just a sign
of the normal ageing process.
≻ IBM certainly makes ageing more difficult, especially from an
energy perspective.
≻ Energy levels normally decline with age and this is exaggerated
by having IBM.
⚂ 2.2.11 My book on IBM.
⚃ In 2023 I decided to write a book focussed on providing information on IBM to patients. Here is the information on the book.
⚁ 2.3 Videos from the Johns Hopkins Myositis Center.
⚂ 2.3.1 Disease Overview.
⚂ 2.3.2 Signs & Symptoms.
⚂ 2.3.3 Lifestyle Options.
⚁ 2.4 Bill's Information pages.
⚂ 2.4.1 Questions to ask your doctor. (LINK to pdf).
⚂ 2.4.2 An information page to take to your family doctor. (LINK to pdf).
⚁ 2.5 Several other diseases we often hear about.
⚁ 2.6 Potential confusion for the doctor.
⚂ 2.6.1 Heart attacks:
⚃ One of the effects of the breakdown of muscle caused by IBM is
that chemicals are released in the blood.
≻ These chemicals include Cardiac Troponin T (cTnT) and creatine
kinase (CK).
≻ The problem arises when a patient with IBM is given a blood test
and these chemicals appear raised – this has traditionally indicated a heart attack.
≻ If the doctor does not know that IBM leads to raising these
levels, it can cause confusion that the patient has had, or is having, a heart attack.
⚂ 2.6.2 Liver tests:
⚃ IBM may cause elevated levels of the liver enzymes, for example,
aldolase, alanine transaminase (ALT) and aspartate transaminase (AST).
≻ These enzymes are released into the blood by damaged muscle
cells, so high levels of ALT and AST may be a sign of liver disease.
≻ Again, if the doctor does not know that IBM leads to raising
these levels, it can cause confusion that the patient has liver issues.
⚂ 2.6.3 Statin-induced muscle disease:
⚃ A rare side effect of the use of statin medications is a muscle
disease called Statin-induced immune-mediated necrotizing myopathy (IMNM), also known as reductase
(anti-HMGCR) myopathy.
≻ This is an inflammatory myopathy
that is not the same as IBM.
≻ However, preliminary research shows that IBM may be seen in some
patients who take / have taken statin medications.
≻ In a study of 221 Idiopathic inflammatory myositis patients, 66
cases were diagnosed with IBM and of these, 20 had taken a statin medication.

⚃ See: Caughey (2018) (LINK to pdf). Also see: 2021 open access article.
⚁ 2.7 “Hereditary inclusion body myopathy” (hIBM) (old terminology).
⚂ Greenberg (2019) pointed out that the group of diseases initially called hereditary inclusion body myopathies, often abbreviated as “hIBM” are entirely different diseases from IBM.
⚁ 2.8 Familial IBM (fIBM).
⚂ Familial IBM (fIBM) is an old term that has been used to refer to
rare cases where IBM is seen in two or more patients within a single generation in a family.
The symptoms and features of fIBM are the same as those seen in IBM.
≻ The familial occurrence of such a rare disorder likely
highlights the importance of genetic predisposition in the causation of IBM.
≻ Should now be called simply IBM.
≻ See: 2.9.
⚁ 2.9 Terminology.
⚂ 2.9.1 Overview of common terms.
⚃ IBM = inclusion body MYOSITIS.
⚃ sIBM = sporadic inclusion body MYOSITIS.
≻ Sporadic means that it just shows up here and there.
≻ This is an older term; it is now recommended “Sporadic” should be dropped.
⚃ fIBM = familial inclusion body MYOSITIS.
≻ Familial means that it shows up in two or more people in the same family in the same
generation.
≻ This is an older term; it is now recommended “familial” should be dropped.
⚂ 2.9.2 Recommended terms.
⚃ The terms “Sporadic IBM,” “Familial IBM,” and “Hereditary Inclusion Body Myopathy” are considered misleading and are no longer recommended.
