Webpage Menu:
⚃ 2.2.5.2 Anti-cytosolic 5'-nucleotidase.
⚃ 2.2.5.1 Creatine kinase (CK), For Background: Creatinine, Creatine, Creatine phosphate (phosphocreatine)
⚄ 2.2.5.1.1 Creatine kinase (CK)
Creatine kinase (CK) is an enzyme found in the heart, brain, skeletal
muscle, and other tissues.
≻ A CK test measures the amount of creatine kinase in the blood.
≻ Increased amounts of CK are released into the blood when there
is muscle damage.
The small amount of CK that is normally in the blood comes primarily
from skeletal muscles.
≻ Any condition that causes muscle damage and/or interferes with
muscle energy production or muscle use can cause an increase in CK.
≻ For example, strenuous exercise and inflammation of muscles,
called myositis, can increase CK as can muscle diseases (myopathies)
such as muscular dystrophy (and IBM).
Elevated CK levels affect enzymes in the liver that are normally used to
test liver function.
≻ A normal CK level with elevated ALT and AST liver enzymes would
suggest a liver problem; a high CK with high ALT and AST levels suggest
muscle problems (with normal kidney function).
⚄ 2.2.5.1.2 Creatinine
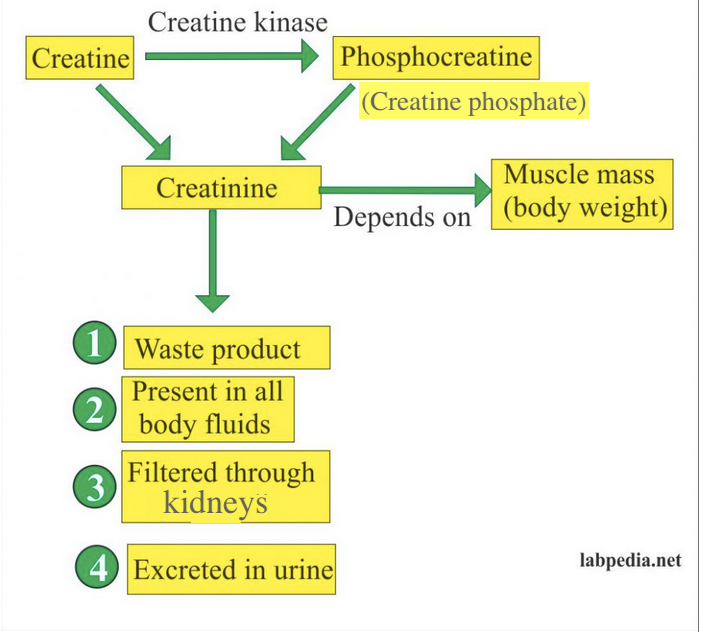
Creatinine [CREE-AT-tin-neen] is a waste product produced by muscles from
the breakdown of a chemical called creatine phosphate from muscle (see
below).
≻ Creatinine is released at a constant rate by the body (depending
on muscle mass).
≻ Creatinine is removed from the body by the kidneys, which filter
almost all of it from the blood and release it into the urine.
The amount of creatinine you produce depends on your body size and your
muscle mass.
≻ For this reason, creatinine levels are usually slightly higher in
men than in women and children (because men usually have more muscle).
A creatinine test measures the amount of creatinine in the blood and/or
urine.
≻ Since almost all creatinine is filtered from the blood by the
kidneys and released into the urine, blood levels of creatinine are
usually a good indicator of how well the kidneys are working.
In a person with normal muscles, a high creatinine level would indicate
potential kidney problems.
≻ In patients with IBM, the muscles are shrinking and creatinine
levels will decline.
≻ Those with higher than usual muscle mass (for example
bodybuilders) or those taking creatine supplements may show higher than
normal creatinine levels (mistakenly suggesting kidney problems).
⚄ 2.2.5.1.3 Creatine
Creatine [CREE-a-teen] is part of the cycle of chemicals that produces energy needed to contract muscles.
Many elite athletes and weight-lifters use nutritional supplements of
creatine (usually taken as creatine monohydrate).
≻ Studies have shown the benefits of dietary creatine
supplementation, which is thought to cause an increase of creatine
phosphate levels in certain types of skeletal muscle fibers.
⚄ 2.2.5.1.4 Creatine phosphate
Creatine phosphate (also known as phosphocreatine) is a slightly different form of creatine that is stored in muscle and used to provide instant energy when muscles need to respond quickly.
⚃ 2.2.5.2 Anti-cytosolic 5'-nucleotidase.
⚃ For an excellent summary see: https://cureibm.org/diagnosis/bloodtests/
⚃ Paul, P., Liewluck, T., Ernste, F. C., Mandrekar, J., & Milone, M. (2021). Anti-cN1A antibodies do not correlate with specific clinical, electromyographic, or pathological findings in sporadic inclusion body myositis. Muscle & Nerve, 63 (4), 490-496. https://doi.org/10.1002/mus.27157.
⚅ Results: Anti-cN1A antibodies were present in 47/92 (51%) patients with sIBM. Comparison of seropositive and seronegative cohorts yielded no significant difference in clinical features, including facial weakness, oropharyngeal and respiratory involvement, or disease severity. The antibody titer did not correlate with the clinical phenotype, CK value, or presence of myotonic discharges on EMG. Anti-cN1A antibody positive patients appeared to have more frequent auto-aggressive inflammation on muscle biopsy but not as an isolated myopathological feature.
⚅ Conclusions: Our study showed that anti-cN1A antibody positive and negative sIBM patients have similar clinical features and disease severity. Anti-cN1A antibodies in our sIBM cohort did not correlate with any studied clinical or laboratory parameter and, therefore, were of limited value in the patient's assessment.
⚃ Lucchini, M., Maggi, L., Pegoraro, E., Filosto, M., Rodolico, C., Antonini, G., Garibaldi, M., Valentino, M. L., Siciliano, G., Tasca, G., De Arcangelis, V., De Fino, C., & Mirabella, M. (2021). Anti-cN1A Antibodies Are Associated with More Severe Dysphagia in Sporadic Inclusion Body Myositis. Cells, 10 (5), 1146. https://doi.org/10.3390/cells10051146
⚅ We did not find significant difference regarding demographic variables, nor quadriceps or finger flexor weakness. Nevertheless, we found that anti-cN1A-positive patients presented significantly lower scores in IBMFRS item 1 (swallowing, p = 0.045) and more frequently reported more severe swallowing problems, expressed as an IBMFRS item 1 score ≤ 2 (p less than 0.001). We confirmed the low sensitivity and high specificity of anti-cN1A Ab in s-IBM patients with a high positive predictive value. The presence of anti-CN1A antibodies identified patients with a greater risk of more severe dysphagia.
⚃ 2.2.5.3 References.
⚃ Felice, K. J., Whitaker, C. H., Wu, Q., Larose, D. T., Shen, G., Metzger, A. L., & Barton, R. W. (2018). Sensitivity and clinical utility of the anti-cytosolic 5'-nucleotidase 1A (cN1A) antibody test in sporadic inclusion body myositis: report of 40 patients from a single neuromuscular center. Neuromuscular Disorders. https://doi.org/10.1016/j.nmd.2018.06.005
⚅ The anti-cN1A antibody test has limited diagnostic utility in IBM.
⚃ Greenberg, S. A. (2017). Inclusion Body Myositis Pathogenesis: Steady Progress. Annals of Neurology . http://doi.org/10.1002/ana.24920
⚃ Researchers' Work from Kumamoto University Focuses on Inclusion Body Myositis (Pathomechanisms of Anti-Cytosolic 5'-Nucleotidase 1A Autoantibodies in Sporadic Inclusion Body Myositis). (2017, May 26). Health & Medicine Week, 1234.
⚃ Tawara, N., Yamashita, S., Zhang, X., Korogi, M., Zhang, Z., Doki , T., . . . Ando, Y. (2017). Pathomechanisms of anti-cytosolic 5'-nucleotidase 1A autoantibodies in sporadic inclusion body myositis. Annals of Neurology, 81(4), 512-525. https://doi.org/10.1002/ana.24919
⚃ Liewluck, T. (2017). Anti-cytosolic 5'-nucleotidase 1A (cN1A) autoantibodies in motor neuron diseases. Neurology, 89(19), 2017-2018.
⚃ Lilleker, J. B., Rietveld, A., Pye, S. R., Mariampillai, K., Benveniste, O., Peeters , M. T. J., . . . van Engelen, B. G. M. (2017). Cytosolic 5'-nucleotidase 1A autoantibody profile and clinical characteristics in inclusion body myositis. Annals of the Rheumatic Diseases, 76(5), 862-868. https://doi.org/10.1136/annrheumdis-2016-210282
⚃ Herbert, M. K., Stammen-Vogelzangs, J., Verbeek, M. M., Rietveld, A., Lundberg, I. E., Chinoy , H., . . . Pruijn, G. J. M. (2016). Disease specificity of autoantibodies to cytosolic 5'-nucleotidase 1A in sporadic inclusion body myositis versus known autoimmune diseases. Annals of the Rheumatic Diseases, 75(4), 696-701. https://doi.org/10.1136/annrheumdis-2014-206691
⚃ Lloyd, T. E., Christopher-Stine, L., Pinal-Fernandez, I., Tiniakou, E., Petri, M., Baer, A., . . . Mammen, A. L. (2016). Cytosolic 5'-Nucleotidase 1A As a Target of Circulating Autoantibodies in Autoimmune Diseases. Arthritis Care & Research, 68(1), 66-71. https://doi.org/10.1002/acr.22600
⚃ Pluk, H., van Hoeve, B. J. a, van Dooren, S. H. J., Stammen-Vogelzangs, J ., van der Heijden, A., Schelhaas, H. J., . . . Pruijn, G. J. M. (2013). Autoantibodies to cytosolic 5'-nucleotidase 1A in inclusion body myositis. Annals of Neurology, 73(3), 397-407. https://doi.org/10.1002/ana.23822
⚃ Larman, Benjamin, H., Salajegheh, M., Nazareno, R., Lam, T., Sauld, J., Steen, H., . . . Greenberg, S. A. (2013). Cytosolic 5'-nucleotidase 1A autoimmunity in sporadic inclusion body myositis. Annals of Neurology, 73(3), 408-418. https://doi.org/10.1002/ana.23840