(Because of the way articles come out, there is some overlap between years.)
⚂ Jensen, K. Y., Jacobsen, M., Schrøder, H. D., Aagaard, P., Nielsen, J. L., Jørgensen, A. N., … Frandsen, U. (2019). The immune system in sporadic inclusion body myositis patients is not compromised by blood-flow restricted exercise training. Arthritis Research & Therapy, 21(1), 293. https://doi.org/10.1186/s13075-019-2036-2
⚃ Conclusion Blood-flow restricted muscle exercise (BFRE) represents a novel approach in the treatment and/or rehabilitation of sIBM patients. The findings from this study suggest that BFRE training is a feasible and tolerable training regime for sIBM patients, since no detrimental or adverse effects on immune system function could be noted following a 12-week training intervention. Further research into the design of specific BFRE training protocols for sIBM patients is needed. In addition, research efforts into the effect of BFRE training on regenerative myocellular markers including stem cell (satellite cell) proliferation and capillary neoformation also seem warranted to gain a deeper understanding of the potential benefits of BFRE intervention in this frail patient population.
⚂ Weihl, C. C. (2019). Sporadic inclusion body myositis and other rimmed vacuolar myopathies. Continuum (Minneapolis, Minn.), 25(6), 1586-1598. https://doi.org/10.1212/CON.0000000000000790
⚃ SUMMARY: Patients with sporadic IBM experience significant morbidity, and the disease is associated with a large unmet medical need. As therapies are developed, improved diagnosis will be essential. Early diagnosis relies on awareness, clinical history, physical examination, laboratory features, and appropriate muscle biopsy processing. Future research is needed to understand the natural history, identify genetic risk factors, and validate biomarkers to track disease progression. These steps are essential as we move toward therapeutic interventions.
⚂ Selva-O'Callaghan, A., Gil-Vila, A., Simó-Perdigó, M., Trallero-Araguás, E., Alvarado-Cárdenas, M., & Pinal-Fernandez, I. (2019). PET Scan: Nuclear medicine imaging in myositis. Current Rheumatology Reports, 21(11), 64. https://doi.org/10.1007/s11926-019-0864-3
⚂ Minniti, M. C., Statkevich, A. P., Kelly, R. L., Rigsby, V. P., Exline, M. M., Rhon, D. I., & Clewley, D. (2019). The safety of blood flow restriction training as a therapeutic intervention for patients with musculoskeletal disorders: A systemat spoiew. The American Journal of Sports Medicine, 036354651988265. https://doi.org/10.1177/0363546519882652
⚂ Lee, J. H., Boland-Freitas, R., Liang, C., & Ng, K. (2019). Sarcolemmal depolarization in sporadic inclusion body myositis assessed with muscle velocity recovery cycles. Clinical Neurophysiology, (xxxx). https://doi.org/10.1016/j.clinph.2019.08.019
⚂ Güttsches, A., Jacobsen, F., Schreiner, A., Mertens‐Rill, J., Tegenthoff, M., Marcus, K., … Kley, R. A. (2019). Chaperones in sporadic inclusion body myositis—Validation of proteomic data. Muscle & Nerve, 17(11), mus.26742. https://doi.org/10.1002/mus.26742
⚂ Henriksson, H., Henriksson, P., Tynelius, P., & Ortega, F. B. (2019). Muscular weakness in adolescence is associated with disability 30 years later: A population-based cohort study of 1.2 million men. British Journal of Sports Medicine, 53(19), 1221–1230.
https://doi.org/10.1136/bjsports-2017-098723
⚂ Takamiya, M., Takahashi, Y., Morimoto, M., Morimoto, N., Yamashita, S., & Abe, K. (2019). Effect of intravenous immunoglobulin therapy on anti-NT5C1A antibody-positive inclusion body myositis after successful treatment of hepatitis C: A case report. ENeurologicalSci, 16(June), 100204. https://doi.org/10.1016/j.ensci.2019.100204
⚂ Dzangué-Tchoupou, G., Mariampillai, K., Bolko, L., Amelin, D., Mauhin, W., Corneau, A., … Benveniste, O. (2019). CD8+T-bet+ cells as a predominant biomarker for inclusion body myositis. Autoimmunity Reviews, 18(4), 325-333. https://doi.org/10.1016/j.autrev.2019.02.003
⚃ CD8+ T cells from sIBM patients overexpress T-bet. Authors present a more detailed and precise phenotype of peripheral blood CD8+ T cells in sIBM patients, thus enhancing understanding of this disease.
⚃ Authors identified and validated a frequency of CD8+T-bet+ cells greater than 51.5% as a diagnostic biomarker specific to inclusion body myositis, compared to myositis control patients, with a sensitivity of 94.4%, a specificity of 88.5%, and an area under the curve of 0.97.
⚃ Authors identifed an activated cell population (CD8+T-bet+ CD57- CD28low CD27low CD127low CD38+ HLA-DR+) which could play a role in the physiopathology of inclusion body myositis, and identify CD8+T-bet+ cells as a predominant biomarker of this disease.
⚂ Knauss, S., Preusse, C., Allenbach, Y., Leonard-Louis, S., Touat, M., Fischer, N., … Stenzel, W. (2019). PD1 pathway in immune-mediated myopathies: Pathogenesis of dysfunctional T cells revisited. Neurology: Neuroimmunology and NeuroInflammation, 6(3), 1-10. https://doi.org/10.1212/NXI.0000000000000558
⚃ T cells, exposed to persistent antigen and inflammatory molecules, may functionally deteriorate, a process called T-cell exhaustion. Exhausted T cells are subject to complex negative regulation involving signaling through multiple receptors that inhibit functional and proliferative responses, which in turn result in ineffective control of the inflammation. The CD28 family member programmed cell death protein 1 (PD1) is the most highly expressed inhibitory receptor on CD8 + T cells during chronic inflammation, and this receptor has a major role in regulating T-cell exhaustion.
⚃ In this study, we hypothesized that persistent antigen presentation in immune-mediated myopathies leads to dysfunctional states of invading T cells. This finding would provide further evidence for a direct recognition of muscular antigens by invading T cells, and a role for T cells in the pathogenesis of these diseases. In addition, we analyzed molecules driving T-cell exhaustion and senescence in skeletal muscle biopsies from IMNM with anti-SRP or anti-HMGCR antibodies and sIBM as well as ICI-associated immune toxicity-related myositis induced by immune checkpoint inhibitors (irMyositis). [irMyositis: myositis induced by immune
checkpoint inhibitors.]
⚃ In this study, we provide systematic evidence of the presence of dysfunctional T cells and activation of the PD1 pathway in IMNM, inclusion body myositis, and immune toxicity-related myopathy. This finding has implications for the understanding of the role of T cells in the pathogenesis of these diseases.
⚃ in this study, we present clear evidence of T-cell exhaustion, and T-cell senescence to varying degrees in all 3 studied myositis entities: … In sIBM, we found high expression of markers for T-cell exhaustion and T-cell senescence. Differences in the duration of disease might interfere with the immune phenotype of the entities studied herein. Taken together, our findings implicate the involvement of muscle-specific T cells with specific phenotypes in the development of sIBM, IMNM, and irMyositis. Activation of coinhibitory receptors could therefore be a viable treatment target in sporadic immune-mediated myositis entities mandating further prospective studies correlating markers of T-cell exhaustion with clinical outcome.
2019: Special section: Highlighted research of particular significance.
⚂ 1 of 3. Benveniste, O.,& Allenbach, Y. (2019). Inclusion body myositis: accumulation of evidence for its autoimmune origin. Brain, 142(9), 2549-2551. https://doi.org/10.1093/brain/awz229DOWNLOAD PDF.
⚃ "(Benveniste and Allenbach, 2019). — Commentary on Greenberg et al., 2019"
⚃ They [(Greenberg et al., 2019).] show that IBM is driven by highly differentiated cytotoxic T cells and that this pathogenesis is unique among idiopathic inflammatory myopathies.
⚃ Greenberg et al. identified a muscle cytotoxic signature and highly differentiated T cell signature present only in IBM. These cytotoxic and highly differentiated cells were CD8+ and killer cell lectin-like receptor G1 (KLRG1) positive.
⚃ KLRG1 is an inhibitory receptor of the C-type lectin-like family. It is used as a marker of terminally differentiated NK and T cells and is strongly induced by chronic viral and other infections. IBM can occur in the setting of viral infection with HIV-1 or human T cell leukaemia virus type 1 (HTLV-1), but in the majority of cases no chronic viral infection is observed. Thus, in IBM, the chronic antigenic stimulation of T cells must come from some as yet unidentified muscle antigens, presumably presented by the myofibres themselves at their surface by major histocompatibility complex (MHC) class I molecules. MHC class I overexpression is in fact one of the hallmarks of IBM pathology. Thus, in IBM it appears that huge antigen stimulation results over time in transformation of naive or early effector memory T cells to TEMRA, which can even give rise to the phenotype of T cell large granular lymphocytic leukaemia.
⚃ Circulating anti-cN1A autoantibodies have been identified, for example, while genome-wide studies show marked association (P less than 10 -33 ) with HLADRB1, an autoimmune haplotype.
⚃ the study does suggest the value of targeting KLRG1+ cells as an IBM therapeutic. In addition to KLRG1 being a marker of presumed pathogenic cells in IBM muscle, the study demonstrated low expression of KLRG1 on lymphoid tissue central memory T cells, which are of paramount importance for infectious disease defence, and low expression on regulatory T cells that help to suppress autoimmunity (Greenberg et al., 2019). We can thus imagine that a targeted therapy for IBM that aims to deplete TEMRA KLRG1+ presumably effector cells (e.g. with a monoclonal antibody) may have a good safety profile in terms of infections and may efficiently tackle one of the key actors in IBM pathophysiology.
⚃ Glossary
⧈ IBM: Inclusion body myositis is the most prevalent myopathy in individuals over 50 years of age. Its unique phenotype with asymmetrical slowly progressive diffuse muscle weakness mainly affecting the quadriceps, hand finger flexors and swallowing muscles is highly indicative of the diagnosis, and should not be confused with a polymyositis (based on inflammatory infiltrates present on muscle biopsy) because of its resistance to corticosteroids.
⧈ KLRG1: Killer cell lectin-like receptor subfamily G member 1 is a lymphocyte co-inhibitory, or immune checkpoint, receptor expressed predominantly on terminally differentiated effector and effector memory CD8+ T and NK cells.
⧈ TEMRA cells: Terminally differentiated effector memory T cells. Human CD8+ T cells are commonly classified into four subsets based on surface expression of the leucocyte common antigen isoform CD45RA and the lymph node addressin CCR7. Naive T cells (CD45RA+/CCR7+) are thereby distinguished from central memory (TCM, CD45RA—/CCR7+), effector memory (TEM, CD45RA—/CCR7-) and TEMRA (CD45RA+/CCR7-) T cells.
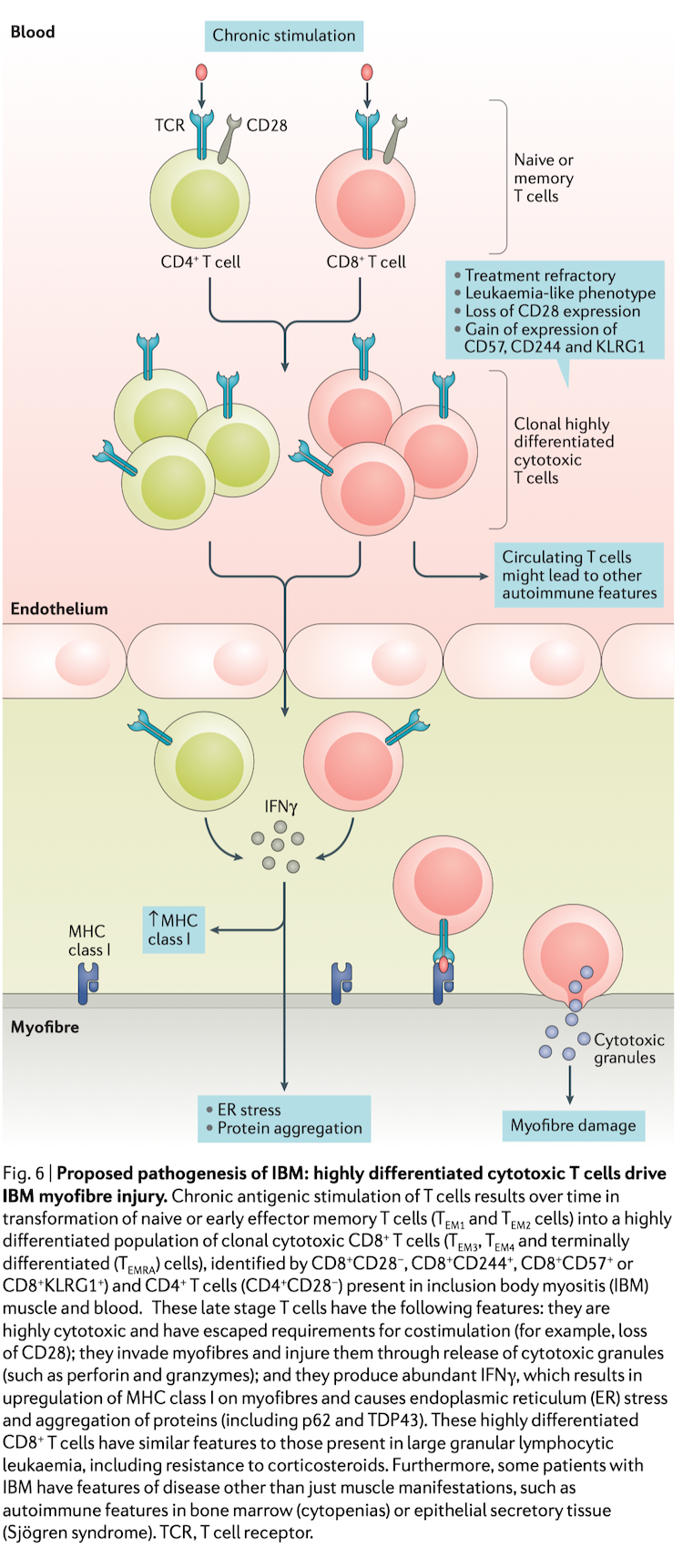
Figure 1 Putative pathogenesis of IBM. CD8+ terminally differentiated effector memory (TEMRA) T cells are activated by their cognate
muscular antigen leading to production of both IFN- (1) and cytotoxic enzymes e.g. granzymes and perforin (2). Cytotoxic enzymes induce
myofibre damage (3). IFN- may lead to mitochondrial dysfunction (4), endoplasmic reticulum stress (5) and also induces MHC-I overexpression
(6). MHC-I overexpression in turn leads to endoplasmic reticulum stress (7). Mitochondrial dysfunction and oxidative stress impair proteasome
function (8). Both endoplasmic reticulum stress and proteasome dysfunction contribute to the accumulation of unfolded and misfolded proteins
leading to rimmed vacuole formation and degenerative features (9).
⚂ 2 of 3. Greenberg, S. A., Pinkus, J. L., Kong, S. W., Baecher-allan, C., Amato, A. A., & Dorfman, D. M. (2019). Highly differentiated cytotoxic T cells in inclusion body myositis. Brain, 1-15.
https://doi.org/10.1093/brain/awz207DOWNLOAD PDF.
⚃ "(Greenberg et al., 2019). — Study"
⚃ Inclusion body myositis is a late onset treatment-refractory autoimmune disease of skeletal muscle associated with a blood autoantibody (anti-cN1A), an HLA autoimmune haplotype, and muscle pathology characterized by cytotoxic CD8 + T cell destruction of myofibres. Here, we report on translational studies of inclusion body myositis patient muscle compared with a diverse set of other muscle disease samples. Using available microarray data on 411 muscle samples from patients with inclusion body myositis (n = 40), other muscle diseases (n = 265), and without neuromuscular disease (normal, n = 106), we identified a signature of T-cell cytotoxicity in inclusion body myositis muscle coupled with a signature of highly differentiated CD8 T-cell effector memory and terminally differentiated effector cells. Further, we examined killer cell lectin-like receptor G1 (KLRG1) as a marker of this population of cells, demonstrated the correlation of KLRG1 gene expression with lymphocyte cytotoxicity across 28870 human tissue samples, and identified the presence of KLRG1 on pathogenic inclusion body myositis muscle invading T cells and an increase in KLRG1 expressing T cells in inclusion body myositis blood. We examined inclusion body myositis muscle T-cell proliferation by Ki67 immunohistochemistry demonstrating that diseased muscle-invading T cells are minimally or non-proliferative, in accordance with known properties of highly differentiated or terminally differentiated T cells. We found low expression of KLRG1 on infectionprotective human lymphoid tissue central memory T cells and autoimmune-protective human blood regulatory T cells. Targeting highly differentiated cytotoxic T cells could be a favourable approach to treatment of inclusion body myositis.
⚃ Here, we report on translational studies of IBM patient muscle and blood samples compared with large numbers of muscle samples from other muscle diseases, identifying a unique cytotoxic lymphocyte signature and a highly differentiated T-cell signature in IBM muscle, highlighting the relevance of highly differentiated cytotoxic T cells to the pathogenesis of IBM. In particular, killer cell lectin-like receptor G1 (KLRG1), an inhibitory T- and NK-cell receptor that is known to mark highly differentiated cytotoxic T cells, is identified on IBM blood and muscle-invading T cells.
⚃ Evaluation of muscle gene expression across 305 muscle biopsy samples from a wide range of muscle diseases, compared to 106 normal samples, showed a cytotoxic lymphocyte signature in IBM distinct from all other muscle diseases, particularly other forms of inflammatory myopathy, which include dermatomyositis, polymyositis, autoimmune necrotizing myopathy, and non-specific myositis.
⚃ To identify potential therapeutic targets that are enriched among human cytotoxic T cells, we examined a genomic dataset (European Bioinformatics Institute, accession ETABM-40) of human blood CD8 + T cell differentiation constructed on sorted CD8 + naive, central memory, effector memory (TEM), and terminally differentiated effector memory (TEMRA) T cells.
⚃ This strategy identified KLRG1 as a marker of T cells that could be potential therapeutic targets.
⚃ Collectively, the current data and previous studies demonstrate that muscle and blood CD4 + and CD8 + T cells in IBM have been driven to highly differentiated effector T cells defined in various overlapping ways, such as loss of CD28, loss of CD62L on CD45RA + T cells gain of CD244, gain of CD57 and gain of KLRG1. These cells have potent cytokine (e.g. IFN-gamma) secreting and cytotoxic capacities. Specifically, IBM blood CD8 + CD28 - T cells have been shown to be major producers of IFN- gamma. These T-cell phenotypic changes are also seen in T cell large granular lymphocytic leukaemia (LGLL), a treatment-refractory expansion of clonal highly differentiated effector CD8 + T cells previously linked to IBM. LGLL T and NK cell expansions are associated with IL-15, and it is notable that IBM muscle has significantly increased IL15 gene expression.
⚃ A major distinction between polymyositis and IBM evident here is the presence of highly differentiated CD8 + CD57 + T cells in IBM muscle but lacking from polymyositis muscle, and the correlation of KLRG1 expression with cytotoxicity present in IBM but not polymyositis.
⚃ These studies highlight possible reasons for IBM treatment-refractoriness and the potential value of targeting the highly pathogenic T-cell population. Molecules highly expressed by these cells, but with lower expression by regulatory T cells and central memory T cells are potential favourable targets for an IBM therapeutic
⚃ Abstract: Inclusion body myositis (IBM) is often viewed as an enigmatic disease with uncertain
pathogenic mechanisms and confusion around diagnosis, classification and prospects for
treatment. Its clinical features (finger flexor and quadriceps weakness) and pathological features
(invasion of myofibres by cytotoxic T cells) are unique among muscle diseases. Although IBM T cell
autoimmunity has long been recognized, enormous attention has been focused for decades on
several biomarkers of myofibre protein aggregates, which are present in less than 1 percent of myofibres in
patients with IBM. This focus has given rise, together with the relative treatment refractoriness of
IBM, to a competing view that IBM is not an autoimmune disease. Findings from the past decade
that implicate autoimmunity in IBM include the identification of a circulating autoantibody
(anti-cN1A); the absence of any statistically significant genetic risk factor other than the common
autoimmune disease 8.1 MHC haplotype in whole-genome sequencing studies; the presence of a
marked cytotoxic T cell signature in gene expression studies; and the identification in muscle and
blood of large populations of clonal highly differentiated cytotoxic CD8+
T cells that are resistant
to many immunotherapies. Mounting evidence that IBM is an autoimmune T cell-mediated disease
provides hope that future therapies directed towards depleting these cells could be effective.
.
⚃ Conclusions: Tremendous progress has been made in the clinical and pathogenic understanding of IBM over the past decade. Major advances in biomarker identification, including the notable whole genome linkage to an HLA autoimmune haplotype, the identification of a specific autoantibody and T cell phenotypical abnormalities, have advanced IBM diagnosis and pathogenic understanding. IBM is unique among muscle diseases owing to its molecular signature involving highly differentiated cytotoxic T cells that have escaped immune regulation. Although viewed as treatment refractory, only very limited therapeutic approaches have been carefully studied to date, and none of these has been rationally directed towards targeting this population of T cells; some treatments (such as corticosteroids and alemtuzumab) have had predictably counterproductive liabilities. Complete understanding of the pathogenesis of IBM, like most acquired diseases in humans, awaits successful therapeutic responses from mechanistically targeted therapies.
———————
⚂ Benveniste, O.,& Allenbach, Y. (2019). Inclusion body myositis: accumulation of evidence for its autoimmune origin. Brain, 142(9), 2549-2551. https://doi.org/10.1093/brain/awz229
⚂ Greenberg, S. A., Pinkus, J. L., Kong, S. W., Baecher-allan, C., Amato, A. A., & Dorfman, D. M. (2019). Highly differentiated cytotoxic T cells in inclusion body myositis. Brain, 1-15.
https://doi.org/10.1093/brain/awz207
⚂ Greenberg, S. A. (2019).
Inclusion body myositis: Clinical features and pathogenesis.
Nature Reviews Rheumatology 2019, 1.
https://doi.org/10.1038/s41584-019-0186-x
⚂ Lilleker, J. B., Rietveld, A., Pye, S. R., Mariampillai, K., Benveniste, O., Peeters, M. T. J., … van Engelen, B. G. M. (2017). Cytosolic 5'-nucleotidase 1A autoantibody profile and clinical characteristics in inclusion body myositis. Annals of the Rheumatic Diseases, 76(5), 862-868. open access https://doi.org/10.1136/annrheumdis-2016-210282
⚂ Ramdharry, G., Morrow, J., Hudgens, S., Skorupinska, I., Gwathmey, K., Currence, M., … Machado, P. M. (2019). Investigation of the psychometric properties of the inclusion body myositis functional rating scale with rasch analysis. Muscle & Nerve, 60(2), mus.26521. https://doi.org/10.1002/mus.26521
⚃ In conclusion, we have presented a Rasch modified version of the clinician rated IBMFRS consisting of an upper limb scale, a lower limb scale, and a 9-item combined scale that can be used with the existing item descriptors. An interval score for each scale has been calculated that can be used in the analysis of the modified IBMFRS when used as an outcome measure.
⚃ See Hanna et al.(2019); The RESILIENT study is valuable for our understanding of the pathology of inclusion body myositis and disease progression over the course of a year. Modulation of the myostatin system in neuromuscular diseases will continue to be investigated, but will not be without hurdles. In that respect, bimagrumab seemed to be safe and well tolerated in the RESILIENT study. For patients with inclusion body myositis, other drugs are awaited—eg, arimoclomol and sirolimus, two drugs that are available orally. Arimoclomol is currently under investigation in clinical trials of inclusion body myositis and amyotrophic lateral sclerosis. This drug's main mechanism of action is enhancement of heat shock protein function that protects cells from stress. Sirolimus is a well established immunosuppressant in transplantation surgery. This drug acts via suppression of the mammalian target of rapamycin and reduces T-cell proliferation. The effect of sirolimus on macroautophagic activity—a central element of muscle degenerative cascades around amyloid precurser protein and beta-amyloidled to initiation of a phase 2 trial in inclusion body myositis, which showed promising results; a larger trial is planned. Along with these and similar approaches, blockade of the myostatin pathway could serve as a potentially useful add-on intervention in future studies. The number of past and ongoing clinical trials in inclusion body myositis provides hope that a beneficial treatment can be identified in the future.
⚂ Furer, V., Rondaan, C., Heijstek, M. W., Agmon-Levin, N., van Assen, S., Bijl, M., … Elkayam, O. (2019). 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Annals of the Rheumatic Diseases, annrheumdis-2019-215882.https://doi.org/10.1136/annrheumdis-2019-215882
⚃ Lists inclusion body myositis as an autoimmune inflammatory rheumatic disease (AIIRD).
⚃ Our aim was to update the present European League Against Rheumatism (EULAR) recommendations for vaccination in patients with AIIRD published in 2011 and to incorporate the new evidence on the incidence/ prevalence of vaccine preventable infections (European League) among AIIRD patients, along with efficacy, immunogenicity and safety of vaccines provided to AIIRD patients under a wide range of immunosuppressive therapies.
⚂ Yamashita, S., Matsuo, Y., Tawara, N., Hara, K., Yamamoto, M., Nishikami, T., … Ando, Y. (2019). CYLD dysregulation in pathogenesis of sporadic inclusion body myositis. Scientific Reports, 9(1), 11606. https://doi.org/10.1038/s41598-019-48115-2
⚃ Dysregulation of CYLD may reinforce myodegeneration in the pathophysiology of siBM by attenuating autophagic clearance of protein aggregates. Regulating CYLD in muscle fibres might serve as a novel therapeutic strategy for sIBM treatment.
⚃ We have demonstrated that CYLD localized in the nuclear and perinuclear regions of degenerative myofibres with rimmed vacuoles in sIBM-affected tissues. CYLD showed localization associated with p-TDP-43, p-p62, and Lys63-linked ubiquitin in the myofibres of sIBM patients and wild-type TDP-43 mice.
⚃ In conclusion, dysregulation of CYLD may reinforce myodegeneration in the pathophysiology of sIBM by attenuating autophagic clearance. Further investigation is required for a better understanding of the role of CYLD in the pathogenesis of sIBM. Regulating CYLD in myofibres might be a novel therapeutic strategy in treating sIBM.
⚂ Hanna, M. G., Badrising, U. A., Benveniste, O., Lloyd, T. E., Needham, M., Chinoy, H., … Amato, A. A. (2019). Safety and efficacy of intravenous bimagrumab in inclusion body myositis (RESILIENT): a randomised, double-blind, placebo-controlled phase 2b trial. The Lancet Neurology, 18(9), 834-844. https://doi.org/10.1016/S1474-4422(19)30200-5
⚃ Bimagrumab showed a good safety profile, relative to placebo, in individuals with inclusion body myositis but did not improve 6MWD. The strengths of our study are that, to the best of our knowledge, it is the largest randomised controlled trial done in people with inclusion body myositis, and it provides important natural history data over 12 months.
⚃ Currently, no evidence is available to support any specific treatment in clinical practice. To date, there are no effective or approved treatment options for inclusion body myositis.
⚂ Suzuki, N., Mori-Yoshimura, M., Yamashita, S., Nakano, S., Murata, K., Mori, M., … Aoki, M. (2019). The updated retrospective questionnaire study of sporadic inclusion body myositis in Japan.
Orphanet Journal of Rare Diseases, 14(1), 155.
https://doi.org/10.1186/s13023-019-1122-5
⚃ "Our multicenter patient and caregiver questionnaire survey revealed that the phenotypes of Japanese patients with sIBM are similar to those of Western country patients with sIBM, at least through a cross-sectional methodology. Many patients described psychological and mental and financial anxiety, given their old age. Thus, a follow-up survey is warranted to determine the prospective natural history of sIBM in Japan."
⚃ Used the Modified IBM Functional Rating Scale (IBMFRS)
⚂ Bhatt, P. S., Tzoulis, C., Balafkan, N., Miletic, H., Tran, G. T. T., Sanaker, P. S., & Bindoff, L. A. (2019). Mitochondrial DNA depletion in sporadic inclusion body myositis.
Neuromuscular Disorders, 29(3), 242-246.
https://doi.org/10.1016/j.nmd.2019.02.001
⚃ "Our findings suggest that mtDNA depletion is a more consistent finding in sIBM, and one that may be implicated in the pathogenesis of the disease."
⚃ Assumes the same disease in the sporadic and hereditary forms - "Inclusion body myositis is usually a sporadic disorder (sIBM) even though a few cases of hereditary (hIBM) cases exist."
⚂ Tsukita, K., Yagita, K., Sakamaki-Tsukita, H., & Suenaga, T. (2018). Sporadic inclusion body myositis: magnetic resonance imaging and ultrasound characteristics.
QJM: An International Journal of Medicine, 111(9), 667-668.
https://doi.org/10.1093/qjmed/hcy065
⚂ Haczkiewicz, K., Sebastian, A., Piotrowska, A., Misterska-Skora, M., Halon, A., Skoczynska, M., … Podhorska-Okolow, M. (2019). Immunohistochemical and ultrastructural analysis of sporadic inclusion body myositis: A case series.
Rheumatology International, 39(7), 1291-1301.
https://doi.org/10.1007/s00296-018-4221-z
⚂ Guimaraes, J. B., Zanoteli, E., Link, T. M., de Camargo, L. V., Facchetti, L., Nardo, L., & Fernandes, A. da R. C. (2017). Sporadic Inclusion Body Myositis: MRI Findings and Correlation With Clinical and Functional Parameters.
American Journal of Roentgenology, 209(6), 1340-1347.
https://doi.org/10.2214/AJR.17.17849
⚂ Ioannis, M., Foivos, P., & Dimitrios, K. (2019). A review on the treatment of sporadic inclusion body myositis with Bimagrumab and Alemtuzumab.
International Journal of Neuroscience, 129(3), 297-302.
https://doi.org/10.1080/00207454.2018.1527329
⚂ Poster session
https://www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2019.199.1_MeetingAbstracts.A4712 American Thoracic Society 2019 International Conference, May 17-22, 2019 - Dallas, TX
C37. SYMPTOMS, PLEURAL DISEASE, BEHAVIORAL SCIENCE, AND OTHER TOPICS
Prevalence and Functional Impact of Diaphragm Involvement in Inclusion Body Myositis
Conclusions: Diaphragm Involvement is frequent in advanced IBM, is related to the disease duration and peripheral muscle weakness, and has detrimental effects on lung function, dyspnea and exercise capacity. Diaphragmatic
and has detrimental effects on lung function. dyspnea and exercise capacity. Diaphragmatic dysfunction should be considered in IBM patients with unexplained dyspnea. Further studies are required to investigate its potential as a therapeutic target
⚂ Roos, A., Preusse, C., Hathazi, D., Goebel, H.-H., & Stenzel, W. (2019). Proteomic Profiling Unravels a Key Role of Specific Macrophage Subtypes in Sporadic Inclusion Body Myositis. Frontiers in Immunology, 10(May), 1-11.
https://doi.org/10.3389/fimmu.2019.01040 In the present study, data from unbiased proteomic analysis highlighted the presence of certain proteins playing decisive roles in immune response to be highly abundant in sIBM patients' skeletal muscle biopsies.. . . we show that several different types of macrophages are actively affecting the immune response in sIBM, via a prominent type I interferon signature among others.
⚂ Amlani, A., Choi, M. Y., Tarnopolsky, M., Brady, L., Clarke, A. E., Garcia-De La Torre, I., . . . Fritzler, M. J. (2019). Anti-NT5c1A Autoantibodies as Biomarkers in Inclusion Body Myositis.
Frontiers in Immunology, 10(April).
https://doi.org/10.3389/fimmu.2019.00745 Conclusions: Anti-NT5c1A has moderate sensitivity and high specificity for sIBM using ALBIA. The presence of anti-NT5c1A antibodies may be associated with muscle weakness. Anti-NT5c1A antibodies were not associated with a specific IIF staining pattern, hence screening using HEp-2 substrate is unlikely to be a useful predictor for presence of these autoantibodies.. . . In summary, we report that anti-NT5c1A autoantibodies as detected by ALBIA have a sensitivity of 48.8percent and a specificity of 91.8percent for sIBM. In addition, IIF on a commercial HEp-2 substrate has no utility in screening for anti-NT5c1A antibodies, and there may be a relationship between antiNT5c1A and higher disease severity. Clinicians should interpret positive anti-NT5c1A results in the context of clinical and pathological findings, and exercise caution when applying this biomarker in patients with IIM and other related conditions, such as SLE. Further research is needed to delineate pathogenic mechanisms (if any) of anti-NT5c1A in sIBM and to investigate correlations between high titer anti-NT5c1A seropositivity and disease characteristics.
⚂ Wang, B., Maxwell, B. A., Joo, J. H., Gwon, Y., Messing, J., Mishra, A., . . . Kundu, M. (2019). ULK1 and ULK2 Regulate Stress Granule Disassembly Through Phosphorylation and Activation of VCP/p97.
Molecular Cell, 1-16.
https://doi.org/10.1016/j.molcel.2019.03.027 data suggest that VCP dysregulation and defective stress granule disassembly contribute to IBM-like disease in Ulk1/ 2-deficient mice. In addition, stress granule disassembly is accelerated by an ULK1/2 agonist, suggesting ULK1/2 as targets for exploiting the higherorder regulation of stress granules for therapeutic intervention of IBM and related disorders.
⚂ Leclair, V., & Lundberg, I. E. (2018). New Myositis Classification Criteria: What We Have Learned Since Bohan and Peter.
Current Rheumatology Reports, 20(4), 18. h
ttps://doi.org/10.1007/s11926-018-0726-4 The new IIM classification criteria are a valuable addition to the myositis disease activity core measures
⚂ Lassche, S., Rietveld, A., Heerschap, A., van Hees, H. W., Hopman, M. TE, Voermans, N. C., . . . Ottenheijm, C. A. (2019). Muscle fiber dysfunction contributes to weakness in inclusion body myositis.
Neuromuscular Disorders, (xxxx), 1-9.
https://doi.org/10.1016/j.nmd.2019.03.001 Both in vivo quadriceps specific force and ex vivo muscle fiber specific force were reduced. Muscle fiber dysfunction was accompanied by reduced active stiffness, which reflects a decrease in the number of attached actin-myosin cross-bridges during activation. Myosin concentration was reduced in IBM fibers. Because reduced specific force contributes to muscle weakness in patients with IBM, therapeutic strategies that augment muscle fiber strength may provide benefit to patients with IBM.
⚂ Kosmidis, M. L., Pikazis, D., Vlachoyiannopoulos, P., Tzioufas, A. G., & Dalakas, M. C. (2019). Trial of canakinumab, an IL-1beta receptor antagonist, in patients with inclusion body myositis.
Neurology - Neuroimmunology Neuroinflammation, 6(4), e581.
https://doi.org/10.1212/NXI.0000000000000581 Conclusions: In this long-term, open-label study, canakinumab showed small, but not clinically appreciable, stabilizing benefits in 2 of 5 patients with sIBM over 1 year, was ineffective in 2 others, and might have worsened one. No patient improved.
⚂ Huntley, M. L., Gao, J., Termsarasab, P., Wang, L., Zeng, S., Thammongkolchai, T., ... Wang, X. (2019). Association between TDP-43 and mitochondria in inclusion body myositis. Laboratory Investigation.
https://doi.org/10.1038/s41374-019-0233-x